Across the world, sport is a ubiquitous human social activity that forms an unique intersection of health, recreation, entertainment, and industry (1). It is both a major economic activity as well as a profound influence on social behavior of individuals at home, work, and play. One practical and concise definition of sport is the organized playing of competitive games according to rules. In that context, rule breaking is cheating to achieve an unfair competitive advantage whether it involves using illegal equipment, match fixing, banned drugs, or any other prohibited means.
The illicit use of banned drugs (doping) to influence the outcome of a sporting contest, constitutes a fraud against competitors, spectators, sport, sponsors, and the public no different from other personal, professional, or commercial frauds. While performance enhancement is almost invariably the intent of cheating, impairing performance is also well known in horse racing and even, rarely, in human elite sports (e.g. drink-spiking of banned drugs, injurious physical assaults). Rules of sporting contest may change by agreement, but once set, represents the boundaries of fair competition. Nevertheless, fairness is an elastic, socially constructed concept which may change gradually over time. For example, a century ago deliberate training itself was considered an ungentlemanly breach of fairness as competition was then envisaged as a contest based solely on natural endowments. Similarly, some sports once maintained a distinction between amateurs and professionals. The philosophical foundations of the concept of fairness is a deep and complex issue (2,3) where the focus has been mainly on distributive justice with an implicit goal of equality of outcomes. Less attention has been given to the philosophical basis of fair competition in sport where the prior distribution of talent and training and the outcome of contest are intended to provide equality of opportunity, but not of outcome, between contestants.
Naïve arguments are made that deny doping is cheating, or unsafe or violates the spirit of sport and asserting that drugs should be freely available or under medical supervision (4-6). However, removing prohibition on doping would immediately render drug taking as pervasive as training in elite sport extending to promising underage and sub-elite athletes. Ensuing demands on doctors to prescribe excessive, often massive, drug doses without medical indications would be unprofessional, unethical, and unsafe. This could convert sporting participation into a potentially dangerous rather than a healthful activity. In practice, creating enforceable boundaries for drugs in sport is unavoidable whether it is prohibition or, even under the most idealistic libertarian scenarios, by age or dosage. Within the limitations of unverifiable self-report regarding an illicit activity (7,8), surveys indicate athletes support antidoping testing mainly to prevent cheating but also to promote safety (9-11). Motivating factors for, and routes by which athletes get involved in doping are complex but include the use of non-banned nutritional supplements as a gateway to doping (12) and the suspicion of athletes or their entourage that their rivals may be using illicit drugs, the so-called “false consensus belief” (7,13-15). These philosophical issues are not considered further here and, recognizing that sport requires concrete, practical decisions, the establishment and enforcement of agreed rules is the basis of fair competition. An excellent discussion of the logic and morality of a decisive antidoping approach from an ethicist with extensive experience in sports anti-doping is recommended (16).
It is well understood that individual human genetic endowments are unequal and, among these, sporting prowess is at least partly genetically determined (17). However, little is still known of the genotype-phenotype correlations that underlie beneficial genetic endowments for sports performance. Natural genetic advantages are recognized in height (tallness for basketball, shortness for jockeys and motor-cycle riders) and hereditary erythrocytosis where a high circulating hemoglobin due to a high affinity erythropoietin (EPO) receptor (18)) for endurance sports, or conversely genetic disadvantage such as the common α-actinin-3 deletion genetic polymorphism which limits anaerobic, explosive power (19). More examples of genetic (dis)advantages for sports performance are likely to be identified as genomics continues to expand our understanding of the biological basis of health, including natural human sporting prowess. In the context of sports doping, however, a person’s genetic endowment is a given creating a natural boundary whereby the use of exogenous drugs or chemicals (including DNA) may constitute drug cheating or doping.
Cheating is as old as sport itself, yet the present endemic of doping using pharmaceutical drugs to boost sports performance is largely a Cold War legacy. Eastern European national doping programs were established by governments aiming to achieve a short-cut propaganda victory over their Western rivals, a challenge quickly reciprocated and then taken up by individual coaches and athletes. Starting with power sports (20), the epidemic became entrenched as an endemic in sufficiently affluent circles. In 1967, following the introduction of anti-doping rules by some sports federations, the International Olympic Committee (IOC) established its Medical Commission, which published their first list of prohibited substances. During the 1970’s the IOC Medical Commission took an increasingly active role by banning androgens which required developing standardized, valid methods to detect and deter androgen doping. After discarding alternatives such as immunoassays and blood sampling, in the 1980s mass spectrometry (MS)-based tests became (21) and remain the standard for detecting synthetic androgens in urine.
In 1999, the IOC established the WADA based in Montreal to be equally supported by governments and sporting organizations with its charter, the WADA Code, representing a harmonized set of global anti-doping rules introduced in 2004, revised in 2009 and 2015 and will be again revised in 2021(22). WADA also publishes an annually updated Prohibited List of Substances and Methods, accredits national anti-doping labs together with their operational anti-doping testing framework, and established the Court for Arbitration in Sport (CAS) to settle anti-doping legal disputes as sport’s “Supreme Court”. The WADA Code has been adopted by over 660 sporting organizations including all Olympic and Paralympic organizations and National Anti-Doping Organizations as well as most non-Olympic International and National Sports Federations. The WADA Code prohibits substances or methods which meet 2 of 3 criteria comprising:
- i.
enhance performance (cheating),
- ii.
harmful to health (safety) or
- iii.
violate the spirit of sport (unsporting).
Although the primacy of penalizing cheating is widely understood, implementing these criteria encounter ethical and practical difficulties in proving ergogenic effects of increasing numbers of illicit and/or non-approved substances. These substances have unknown safety so that human testing is not feasible making athlete safety an important consideration. Crucially, the Code imposes strict liability on individual athletes so that a positive anti-doping test (including refusal or avoidance of testing or possession, attempts, trading and tampering with banned drugs) constitutes an anti-doping rule violation (ADRV), regardless of intent or negligence. Sanctions involve suspension from any elite competitive sport and extend to support personnel and teams. Suspensions, once 2 years are now 4 years since adoption of the 2015 Code. This is generally believed to be longer than the ergogenic benefits of doping, although recent evidence suggests that androgen effects on muscle may create durable or even permanent effects (23) which might argue for much longer or permanent banning of androgen doping violators.
The Prohibited List bans, at any time either in or out of competition, the use of performance enhancing hormones, including androgens, EPO and growth hormone and related substances or drugs which stimulate endogenous production of these hormones (Table 1). Among the 15 categories of prohibited substances (12) and methods (3), hormones feature prominently in S1 (anabolic agents, mainly androgens), S2 (peptide hormones, growth factors, related substances and mimetics), S4 (hormone and metabolic modulators), and S9 (glucocorticoids) with S1 and S2 having important “catch-all” provision for unnamed but related substances “with similar chemical structure or biological effects”. In addition, the S0 category bans non-approved substances, those without current regulatory approval for human therapeutic use. The prominence of hormones is reinforced by the WADA laboratory statistics for anti-doping tests where hormones remain the most frequently detected banned drugs (Table 2). In 2017, of over 322,000 anti-doping tests ~1.5% were positive with 61% due to hormones, the vast majority (~99%) due to androgens. These findings confirm that the detection of androgen doping is effective whereas the low rate of detection of hemoglobin or growth hormone doping may reflect the limitations of available tests for peptides and peptide hormones which require blood rather than conventional urine sampling and feature low sensitivity and brief windows of detection, rather than their lack of abuse. Further use of out-of-competition testing and blood samples together with more sensitive detection tests with longer windows of detection are required particularly for peptide hormones.
The prevalence of doping in elite sports as an illicit activity with drastic consequences for athletes admitting guilt remains difficult to quantify using laboratory-based testing, inference from performance, or self-report questionnaires (24). The most promising methods appear to be questionnaires using the unrelated question random response methodology (25). This methodology was developed to estimate the prevalence of sensitive, disapproved, or illicit activities by asking the sensitive personal questions masked by mixing them with unrelated non-sensitive questions in an anonymized framework. This provides overall prevalence self-report estimates of the target activities without allowing for individual identification of answers. One study of two elite athletic competitions provided estimates of 43.6% and 57.1% for recent (last year) and 70.1% of ever use of banned doping methods (26). However, another study using the same methodology found markedly lower prevalence estimates of 0.7% to 11.9% for recent use of banned doping (27). The discrepancies between these prevalence estimates requires further clarification. A significant limitation of these methods is their reliance on athlete’s perception of banned methods. For example, whether “banned drugs” are interpreted as including the widely used (but non-banned) nutritional supplements which athletes are urged to avoid for fear of adulteration with unlabeled banned substances.
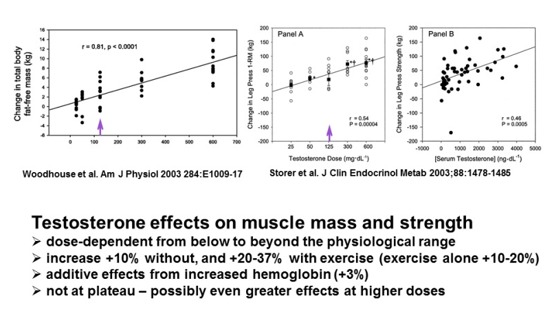
Although the ergogenic effects of androgens were discovered empirically soon after the identification of testosterone as the principal male androgen of testicular origin in 1935 (31), their applications to elite sport performance were mainly developed during the Cold War by trial and error experiments undertaken on unknowing elite athletes (20,32,33); however, the scientific basis of androgen doping was only objectively proven in the 1990’s. Until that time, the settled consensus was that exogenous androgens had no effect in eugonadal men whose androgen receptors were already saturated by endogenous testosterone (T) (20,34,35). The then alleged benefits of androgen doping were misattributed placebo responses together with training and nutritional effects. Using an exemplary placebo-controlled, randomized clinical trial design with a wide range of testosterone doses, Bhasin et al showed that T increased muscle mass and strength in eugonadal young men to a similar extent as exercise alone and with additive effects when combined with exercise (36) (). Subsequent dose-response studies showed that administration of T increased muscle mass and strength by 10% without and 20-37% with exercise (where exercise alone increased them by 10-20%) together with additive effects from 3% increase in circulating hemoglobin. These benefits extended from below to well above physiological T doses or blood levels without evidence of plateau (37,38) and regardless of age (39).
Androgen doping may be either direct or indirect (Table 3, ). Direct androgen doping involves administration of testosterone, natural or synthetic androgens whereas indirect androgen doping includes a variety of non-androgenic drugs which increase endogenous T. Direct androgen doping originally involved all pharmaceutically marketed natural (T, DHT, nandrolone) and synthetic androgens but has extended to non-marketed designer and nutraceutical androgens as well as pro-androgens (androstenedione, DHEA) and the new class of non-steroidal androgens (selective androgen receptor modulators, SARM (40)). Indirect androgen doping involves use of hCG, LH, anti-estrogens (estrogen receptor blockers, aromatase inhibitors), opioid antagonists, and neurotransmitters involved in neuroendocrine regulation of endogenous LH and T secretion (41-44).
Detection of direct androgen doping using steroids of known chemical structure is highly effective using gas or liquid chromatography MS (45-47). Traces of synthetic androgens or their metabolites may remain detectable for periods up to months after last administration (48). Recent developments including the identification of long-term metabolites has further widened the detection windows for synthetic androgens (49-55). Challenges to detection of synthetic androgens have included the development of non-marketed designer and nutraceutical androgens, the use of natural androgens, and pro-androgens, masking methods, restricting use to out-of-competition training or micro-dosing. Designer and nutraceutical androgens are typically non-marketed synthetic androgens based on structures and synthesis methods recovered from expired patent literature of the 1960-70’s. These are now synthesized by unregulated chemical manufacturers without Good Manufacturing Practice (GMP) licensing advertising and sold over the internet or over-the-counter as nutritional supplements, which may contain undeclared steroids (56). However, once the chemical structures of any synthetic androgens are known, they are easily detectable although the sheer profusion of such chemicals represents an ongoing challenge. Nevertheless, despite their novelty, there is little evidence designer androgens have been used after they are discovered so that there is a high likelihood of detection. As a result, virtually all ongoing androgen ADRVs are still due to conventional marketed synthetic androgens.
Distinguishing Between the Exogenous and Endogenous Steroids
Administration of natural androgens (T or DHT) or pro-androgens (androstenedione, DHEA), raises the problem of distinguishing between the exogenous and endogenous steroids. Exogenous T administration can be detected by the urine T/E ratio, the ratio in urine of T to its 17α-epimer epitestosterone (E), operating as a sensitive screening test. In males, both T and E are co-secreted by Leydig cells and excreted in urine consistently so that the urine T/E is usually stable for any individual over time, being typically around 1. Administration of exogenous T, which is not converted to E, increases the urine T/E ratio and, when it exceeds a specified threshold, is evidence for administration of exogenous T. The urine T/E ratio thresholds were originally population-based, set initially at 6 and then subsequently lowered to 4. However, the urine T/E ratio is not an effective screening test for testosterone doping in females (57) because, unlike males whose circulating testosterone originates from as single source subject to strong negative hypothalamic feedback, circulating testosterone in females originates from three steroidogenic sources (adrenal, ovary, extraglandular conversion) none of which are subject to strong negative feedback by testosterone. Furthermore, the possibility of false negatives and false positives of population-based thresholds are limitations which may require further analysis to confirm or refute T doping in individual cases. These considerations have led to establishment of the steroid module of the Athletes Biological Passport (ABP), a compendium of serial observation of any individual’s tests which creates adaptive individual-specific T/E ratio threshold (58). This substitution of an individual’s own person-specific, in place of the population-based, thresholds allows for more sensitive and accurate detection of individual deviations in urine T/E ratio as evidence of T doping.
One limitation of the urine T/E ratio is a genetic polymorphism of the uridine 5'-diphospho-glucuronosyltransferase (UGT) 2B17 gene which encodes a phase II hepatic enzyme that glucuronidates T rendering it more hydrophilic to facilitate urinary excretion. This polymorphism comprises a genetic deletion which, in homozygotes, produces a non-functional enzyme that reduces urinary T (but not E) excretion to near zero producing an extremely low T/E ratio (<0.1). While this genetic polymorphism has no apparent biological effect on T action, it is unevenly distributed geographically being much more frequent in South East Asian populations (59). This biological false negative means that administration of exogenous T will be greatly reduced and may not exceed the usual population-based T/E ratio thresholds (60). On the other hand, it will exceed any individual’s own specific urine T/E ratio threshold so that genotyping and/or Bayesian profiling of serial T/E ratio in an ABP program provide complementary evidence (61-63).
Administration of exogenous T may also be identified by carbon isotope ratio MS (CIRMS) that can distinguish endogenous from exogenous T according to the C13/C12 ratio of urinary T (64,65). Commercially, steroids are manufactured from plant sterols produced by photosynthesis that exhibit distinctly lower C13/C12 ratio (typically, -26‰ to -36‰ relative to the global standard) compared with mammalian T biosynthesis (between -16‰ to -26‰) (66,67). Hence, a significantly lowered (“depleted”) C13/C12 ratio of urinary T, exceeding 3‰ relative to endogenous reference steroids, indicates that urinary T originates at least partly from exogenous chemical manufacture from plant sterols. CIRMS can also be applied to detect administration of other natural androgens or pro-androgens including DHT and DHEA (68), androstenedione, or even attempted masking by administering E (to lower urine T/E ratio) (66). A few T products (<5% (69)) have recently emerged with a lower, more mammalian-like C13/C12 ratio for urine T (70) creating a challenge for CIRMS detection. Nevertheless, extended isotope profiling of other steroid precursors and metabolites provides additional complementary reference biomarkers (71). A longitudinal application of CIRMS along the lines of another module of the ABP has been proposed (72). Furthermore, development of hydrogen ion ratio mass spectrometry has further enhanced the ability to distinguish between endogenous and exogenous steroids even when the carbon isotope ratio is non-informative (73-75). Suppression of urine (or serum) LH excretion may also provide corroborative evidence for the use of exogenous T or other synthetic androgens (63,76-78).
While MS is highly effective for detecting specific androgens, it requires knowledge of the chemical structure to be detected and otherwise cannot be applied. This principle applies to never-marketed designer or nutraceutical androgens sold over the internet or in unregulated over-the-counter nutritional supplements with unlabeled steroid content. A potential solution is the modern in vitro androgen bioassay that incorporates the human androgen receptor together with a convenient transactivation chemical read-out signal into a host yeast or mammalian cell (79). This has the generic capacity to detect all bioactive androgens regardless of structure due to their direct activation of the androgen receptor. Constructed in vitro androgen bioassays feature a sensitive dose-response signal proportional to the potency of the bioactive androgen (80-83). Yeast host cells have high specificity for detecting androgens but are less sensitive than mammalian cells, which express native steroid mechanisms including steroidogenic enzymes and/or other steroid receptors. Mammalian in vitro androgen bioassays can also detect pro-androgens, steroids lacking intrinsic androgenic bioactivity but which are converted into androgens within the mammalian cell. Hence, while mammalian host cells sacrifice specificity for higher sensitivity, they can also detect pro-androgens (79). Hence yeast and mammalian in vitro androgen bioassays are complementary in detecting both androgens and pro-androgens. The limitations of in vitro androgen bioassays are their susceptibility to matrix effects and difficulties in standardizing bioassay-based test. Consequently. they are best deployed to characterize products and substances for androgens or pro-androgen content rather than to detect androgens in complex biological samples. Hence the yeast androgen bioassay was decisive in the first conviction for use of a designer androgen by proving that tetrahydrogestrinone (THG) was a potent androgen (84) and has also been used to screen synthetic progestins to show that, unlike the original androgen-derived progestins, the modern generation of progestins are not androgenic (85).
Additional underutilized options to detect androgen doping is the use of alternative biological matrices such as hair, skin or nails as well as saliva and exhaled breath (86). Hair has the advantages of minimally invasive sampling with simple, convenient storage and the potential for very long window of detection, according hair growth rates (87). MS-based methods have been reported to detect exogenous (88-102) and endogenous (91,103-106) androgens in human hair following long-term, but not single dose (107), exposure. However, hair analysis tests have yet to undergo the rigorous standardization and validation required to become acceptable anti-doping tests in their medicolegal context. Problems that remain to be fully overcome include matrix effects, low recovery and limited sensitivity as well as the impact of age, hair color, alopecia, and shaving or passive chemical (cosmetic) contamination of hair. Additionally nails and skin could also provide analogous information on past androgen exposure with relatively long windows of detection but suitably rigorous tests are yet to be convincingly developed (108). Saliva sampling has also been considered (109,110) for anti-doping application analogous to the use of salivary cortisol measurement for diagnosis of hypercortisolism (111). While potentially applicable to xenobiotic drugs, salivary testosterone immunoassay is not sufficiently accurate (112) and is not suitable to detect testosterone doping because even microscopic blood contamination (e.g. gingivitis, chewing hard food, tooth brushing) produces anomalous high readings. The existence of these renders salivary testosterone testing for antidoping purposes as unreliable by providing opportunity for claims of false positive for any adverse findings. Exhaled breath testing has also been investigated for certain small molecular weight chemicals (113). In theory, androgen-induced gene expression in circulating leukocytes might provide an additional biomarker of androgen action if specific and reproducible signatures can be defined (114); however, as direct detection of androgens is feasible and preferable for proving an ADRV, a role for gene expression biomarkers of androgen action remains to be established for anti-doping.
Hemoglobin doping involves either direct blood transfusion or indirect methods of increasing hemoglobin via stimulating erythropoiesis by administration of erythropoietin, its analogs or mimetics (see excellent reviews (121,122)) (Table 4). Boosting hemoglobin is advantageous in aerobic, endurance sports such as road cycling, distance running and cross-country skiing. Maximal oxygen consumption (Vo2), a rate-limiting factor in aerobic exercise, principally determined by cardiac output and blood oxygen transfer with a lesser contribution from tissue oxygen transfer (123). Experiments on exercise tolerance and blood transfusion were first reported in 1945 (124,125) but the scientific basis of hemoglobin doping via enhanced tissue oxygen transfer was firmly established in 1972 by the work of Ekblom et al reporting experiments in healthy volunteers who underwent venesection and/or re-transfusion of 1, 2 or 3 units (400 mL) of blood with repeated testing of maximal exercise-induced oxygen consumption before and after each procedure (126). This proved unequivocally that the maximal oxygen consumption was highly correlated with acute changes in hemoglobin (). Subsequently, during the 1970-80’s before its banning in 1988, blood transfusion became a prevalent surreptitious practice in road cycling and cross-country skiing and the apparently low prevalence among distance runners may be an underestimate (127). Modelling of historical performance in European road cycling from 1993 onwards shows a unique progression averaging an improvement of 6.4% corresponding closely with the performance enhancement (6-7%) due to rhEPO administration, which is sustained for at least 4 weeks after administration (128-130).
Autologous Transfusion
The biggest gap in current anti-doping tests is the lack of a specific test to detect autologous transfusion (138). Research to identify robust physico-chemical or biological markers for direct identification of a subpopulation of ex-vivo aged erythrocytes is underway using flow cytometry (139) but the dilution and rapid clearance of effete erythrocytes make for challenging detection problems (140). In the interim, other indirect methods have been developed. These include measuring urinary excretion of phthalates, plasticizers that leach out from the polyvinylchloride blood packs used to store venesected blood (141). This test has brief window of detection (2 day) so will detect auto-transfusion during or immediately before events (characteristic in road cycling, according to convicted dopers) but may miss earlier auto-transfusion. Furthermore, the ubiquity of low-level environmental phthalate exposure requires establishing detection thresholds and non-plastic blood containers can be used. An alternative is the measurement of total hemoglobin mass (142), a measure with good stability and reproducibility even during exercise and circumvents influence of variations in plasma volume such as due to dehydration or dilutional masking (142,143). However, as this requires inhalation of carbon monoxide, which has transient detrimental effects on performance, it is not ideal for routine anti-doping use and its sensitivity may be insufficient to detect all EPO micro-dosing (144,145). Nevertheless, alternative methods for serial measurement of total hemoglobin mass remain attractive. Other hypothetical methods include the detection of microRNA (146) or immune reactions to transfusion (147) but the sensitivity and specificity of these proposed tests remains to be fully evaluated.
The best detection test for autologous hemoglobin doping at present is the hematological module of the ABP introduced in 2009 (148). Conceptually, it is a biomarker test which adopts a Bayesian approach of creating serially-adaptive, person-specific reference limits, based on using all prior testing, to supplant population-based thresholds. Combining all of an individual’s previously collected hematological data creates a probabilistic test of whether any new result deviates significantly from that individual’s personal reference limits (149). These person-specific thresholds allow for ongoing refinement and reinforcement by further testing. The thresholds are calculated by a variety of algorithms incorporating routine hematological parameters, notably hematocrit and reticulocyte counts. Those were developed over the last two decades to create the ABP hematological model which is sensitive to both direct and indirect hemoglobin doping (150). The first attempts to regulate hemoglobin doping in the late 1990’s sought to prevent road cyclists or cross-country skiing athletes competing on health risk grounds when their hematocrit exceeded pre-determined, population-based safety criteria (e.g. hematocrit 0.50 or hemoglobin 170 g/L for cycling). However, while this excluded extreme hemoglobin doping only until the short period when the safety threshold was no longer exceeded, it allowed an increase in an athlete’s natural hematocrit, typically averaging ~0.45, up to the permitted ceiling threshold which fostered titrated hemoglobin doping and manipulations like hemodilution by saline or plasma volume expander infusions to avoid detection (151). More sophisticated hematological algorithms were then developed to detect hemoglobin doping initially for the Sydney 2000 Olympics (152,153), the first generation of algorithms developing validated tests for ongoing and for recent cessation of hemoglobin doping, using a combination of biochemical variables related to erythropoiesis physiology. This approach was simplified by a second generation algorithm using only routine hematological parameters (hemoglobin, reticulocytes) (154), and was subsequently combined with the concept of a sequential development of individual-specific reference ranges (155) into a third generation algorithms (156,157) which were refined for the ABP (148,149). The hematological module of the ABP currently employs an algorithm involving 8 parameters derived from routine hematological profile (hemoglobin, hematocrit, erythrocyte count, reticulocyte count and percentage, mean corpuscular volume, mean corpuscular hemoglobin, mean corpuscular hemoglobin concentration) (158). This is capable of detecting any form of hemoglobin doping, whether direct or indirect, with good but imperfect sensitivity (143-145) and using only routine hematological tests. The reported increasing use of very low EPO doses (“micro-dosing”) would markedly reduce the magnitude of any dose-dependent ergogenic benefits (145) while still carrying risks of detection, disqualification, and disgrace.
Stimulation of Erythropoiesis
Indirect methods to increase hemoglobin include administration of recombinant human EPO or its analogs as well as hypoxia-mimetic drugs (hypoxia-inducible factor stabilizers, iron chelation, cobalt, 2,3 diphosphoglycerate analogs) or artificial oxygen carriers (perfluorocarbons, hemoglobin-based oxygen carriers). Related but non-banned methods include altitude training or its simulation by sleeping in hypoxic rooms which are less effective than hemoglobin doping (129).
The identification of the human EPO gene in 1985 led to the marketing of recombinant human EPO (rhEPO) between 1987-9. Despite the IOC’s prohibition of EPO’s use in sports in 1990, the commercial availability of rhEPO created powerful new opportunities for indirect hemoglobin doping which were soon proven experimentally (159). A drug, which circulates for hours to days, but with potent and long-lasting ergogenic effects after its disappearance due to the 4-month lifespan of erythrocytes, is both attractive for doping and a challenge to anti-doping testing. Expiry of the rhEPO patent in 2004 allowed marketing of a profusion of generic EPO (“biosimilar”) products, estimated globally at over 80 (160), as well as modified EPO analogs (darbepoeitin, pegylated EPO, peginesatide, EPO fusion proteins). A fatal cluster involving deaths of 18 Dutch and Belgian road cyclists, presumably due inadvertent over-dosage during empirical attempts to maximize ergogenic effects of illicit rhEPO, was reported (161), although difficult to verify (162). A similar excess of unexpected deaths of road cyclists was also reported again in 2003-5 when novel EPO analogs and EPO biosimilars were marketed.
Detection of EPO in urine is difficult because of the prevailing low concentrations and need to distinguish exogenous recombinant from endogenous EPO. The first effective method for rhEPO in urine was a double immunoblot (163,164) which was capable of detecting urinary excretion of a variety of exogenous EPO products and analogs according to their differences in glycosylation side-chains, and differences in primary amino acid sequence where they exist, while distinguishing them from endogenous EPO. Although further refined (165) and extended to other EPO analogs (166), the immune-electrophoresis test is sensitive but relatively laborious and provides only a short window of detection of up to a week post-administration (167). More sensitive methods based on proteomics (for EPO analogs with differences in primary structure) together with glycomics (for biosimilars and analogs which have host-cell specific variations in side-chain glycosylation but unchanged natural EPO primary structure (168)) are possible but not yet approved. Additional applications to detect EPO and analogs using dried blood spots have been reported (169). Similarly, preliminary investigations have proposed a EPO-induced gene expression signatures as a biomarker to detect EPO administration but specificity relative to exercise and other physiological effects remain to be clarified (170).
Other EPO mimetics such as hypoxia mimetic drugs including hypoxia-inducible factor (HIF) stabilizers and related small molecules represent growing threats as potential indirect hemoglobin doping agents (171). These non-peptide chemicals interfere with various steps of the molecular oxygen sensing mechanism to mimic renal hypoxia and thereby induce EPO secretion resulting in increased blood hemoglobin. As a convenient orally active alternative to the lucrative pharmaceutical market for injectable erythropoiesis-stimulating peptides (~$7-8 billion (172)) to counteract anemias of chronic renal failure or marrow failure due to myeloproliferative disease or cytotoxic cancer therapy, they constitute a very active area of pre-clinical patent-based clinical drug development (171). Experience suggests that such innovator products can enter the doping black market before marketing approval (150,171). Despite the profusion of pre-clinical leads, they represent families of related chemical structures disclosed in patents for which LC and/or GC-MS detection tests should, in principle, be effective. Understanding the metabolism of these drugs when they come to market may identify long-lasting metabolites that can extend the windows of detection. Coupled with evidence from the ABP, manipulation of the EPO pathway may be detected in conjunction with corroborative measurement of inappropriately suppressed or elevated endogenous EPO for the prevailing hemoglobin level.
HIF is a key generic biological mechanism for tissue sensing of hypoxia and triggering local (neovascularization, angiogenesis) and systemic (EPO) defensive reactions. The promoter of the EPO gene contains enhancer and inhibitor regions with the hypoxia-responsive element which binds HIF and a GATA binding site which enhance and inhibit, respectively, EPO gene transcription. HIF is a heterodimer formed by constitutively expressed subunits with the β subunit in excess and availability of α subunit limiting formation of bioactive HIF. The 3 HIFα subunit isoforms are subject to hydroxylation of specific proline residues by prolyl hydroxylase enzymes which inactivate HIFα by ubiquitination, a tag which targets it to proteasomal degradation. HIFα subunit inactivation is strongly dependent on tissue oxygenation being active during normoxia but reduced during hypoxia when persistence of HIFα stabilizes the HIF heterodimer. Notably, during hypoxia the expression of HIFα in renal cortical cells stimulates EPO gene expression so that HIF stabilization by prolyl hydroxylase inhibitors leads to increased EPO secretion and circulating hemoglobin. Hence inhibiting prolyl hydroxylase activity via blocking its required cofactors (ascorbate, ketoglutarate, iron) using cobalt, nickel, iron chelation, ketoglutarate analogs or mechanism-based chemical inhibitors can result in increased hemoglobin via stimulation of EPO secretion (171). Similarly, small molecule GATA inhibitors potently stimulate circulating EPO, hemoglobin and performance in mice (173) although none have yet been marketed so their human efficacy and safety remain to be determined.
Another approach to increase oxygen delivery to muscle has been to exploit the ability of 2,3 diphophoglycerate (2,3 DPG), whose binding to hemoglobin reduces its affinity for oxygen with the left-shift of its oxygen dissociation curve as an oxygen unloading mechanism in tissues. 2,3 DPG analogs, developed as radiation sensitizers for hypoxic radio-resistant tumors, enhance tissue oxygen delivery in vivo (174,175) but would feature only short-term, acute effects readily detectable by mass spectrometry (176,177).
Adverse effects from use of rhEPO or its analogs are well known in medicine but poorly recognized in doping. They include immunogenicity (with risk of EPO autoantibody mediated pure red cell aplasia) (178,179), cardiovascular complications (including venous thromboembolism, stroke, hypertension and myocardial infarction) and premature death (180-183). In routine clinical use of EPO to correct renal anemia, the goal is a gradual increase to subnormal hemoglobin targets so that the excessive and/or rapid rises in hematocrit and blood viscosity (184) may explain the excess unexplained deaths among young European road cyclists in the late 1980s. In addition, use of rhEPO may deplete iron stores which limits hemoglobin synthesis so that athletes may also use oral or injectable iron supplements, which carry their own risks such as iv iron supplementation’s potentially adverse effects in enhanced tissue oxidative damage and excess mortality in chronic kidney disease (185). Although clinical safety experience with ESAs is restricted to patients with serious medical disorders, there is evidence from the general community that higher natural hematocrit is associated with worse long-term cardiovascular health outcomes (186-188).
Growth hormone (GH) is a tissue growth promoter in children but after puberty it is predominantly a metabolic hormone although latent tissue growth promoting effects may be unleashed under non-physiological circumstances, such as during recovery from tissue injury. There is consistent anecdotal evidence that GH has been used in elite sports for decades (189). Nevertheless, ergogenic effects of GH remain unproven and largely speculative as discussed in excellent recent reviews (190-192). Claims of GH benefits in sport have included increases in muscle mass and strength, especially in conjunction with androgens, and/or improved tissue healing with more rapid recovery from either major injuries or minor repetitive injuries, such as from intense physical training allowing for more effective training. The biological basis of ergogenic effects of GH have been tested in these two different scenarios with largely inconclusive findings.
Evidence for direct enhancement of athletic performance by GH has been investigated in two well controlled RCTs with a primary focus on athletic performance. In one study, 96 recreational sub-elite athletes (63 male, 33 female, mean age 28 years) were administered 8 weeks of daily sc injections of GH or placebo with the men also having weekly im injections of T enanthate or saline placebo for the last 5 weeks (193). GH increased lean (muscle) mass (by +2.7 kg) and reduced fat mass (by -1.4 kg) while T increased lean mass (alone by +2.4 kg, by +5.8 kg with GH). The effects of GH were marginally significant for anaerobic sprint capacity (by +3.9%, p=0.05) when pooling male and female participants but this was due to significant effects in men only (by +5.5% alone and +8.3% with GH). However, there were no significant effects on maximal Vo2 consumption, dead lift, or jump height (193). A second study involved 30 healthy non-athletes (15 male, 15 female, mean age 25 years) who were administered daily sc injections of GH at high (4.6 mg/day) or low (2.3 mg/day) doses or placebo (194). There was no significant effect on muscle mass or maximal Vo2 consumption. Additional controlled studies of GH effects but with less focus on athletic performance have also shown that (a) a single dose of GH (~0.8 mg) in 9 recreational athletes did not affect maximal Vo2 or power output in repeated 30 min bursts of bicycle ergometry (195), (b) short term (6 days), low dose GH (~1.7 mg/day) treatment of 48 male androgen abusers withdrawn from androgens for 12 weeks significantly increased maximal Vo2 more than placebo (196), (c) daily sc injections of a GH receptor antagonist (pegvisomant) or placebo for 16 days to 20 sedentary men did not change maximal Vo2 although time to exhaustion at 90% maximal Vo2 was reduced (197) and (d) 4 weeks of daily sc injections of GH (~5 mg/day) increased whole body protein synthesis (198), lipolysis and glucose uptake (199) with uncertain significance for athletic performance. Overall, these studies indicate that GH has, at most, a modest ergogenic effect in men only and through enhancing T effects. That is consistent with the fact that young women have markedly greater growth hormone secretion than young men so that growth hormone cannot explain the sex differences in athletic performance (200).
It is also claimed that GH may enhance injury healing, thereby facilitating more intensive training and/or recovery from muscle, connective tissue or bone injury, notably in contact sports. This claim is difficult to evaluate and no well controlled studies of recovery from sports injuries or tolerance of training intensity in elite athletes are reported. The most germane surrogate evidence available arises from investigations on the use of GH in recovery from injuries due to burns, fracture, or for wound healing. A recent Cochrane meta-analysis review of GH treatment effects on recovery from burns injury and healing of donor skin graft sites suggests that GH has a small benefit in skin healing with large burns and reduced hospital stay but there was no benefit in reducing mortality or scarring and adverse effects, notably hyperglycemia, were increased (201). In practice, the increased mortality due to administration of high dose GH in critical illness (202) has led to GH treatment not being widely adopted in clinical practice of treatment of burns. Similarly, the only well controlled study of GH effects on bone healing from fracture reported that, among over 400 patients with tibial fractures treated for up to 16 weeks with GH (1, 2 or 4 mg/day) or placebo, there was no benefit of GH for overall healing (203). Finally, while there are numerous experimental studies of GH or growth factors on wound healing in animal models a wide variety of findings are reported with detrimental, neutral, or beneficial effects but no well-controlled human studies are available. In summary, the available evidence for improved tissue repair or regeneration is minimal.
Important caveats on interpreting these few well designed studies are that the effects of higher GH and T doses, as used in doping, have not been studied so that more potent higher dose and/or interactive effects cannot be excluded in the absence of well controlled, high dose, placebo-controlled studies. Nevertheless, the hypothesis that high dose GH exposure would enhance muscular function is inconsistent with the experience of acromegaly in which patients experience much higher (25-100 times) growth hormone exposure than doses that can be ethically administered to healthy human volunteers (204), yet characteristically display muscular weakness rather than increased muscle size or strength (205). Anti-doping science history suggests that caution is required before rejecting evidence for claimed ergogenic effects without investigations replicating the pharmacological doses used.
Furthermore, safety analysis is not feasible based on the few, small, short-term studies of GH’s potential ergogenic effects; however, there are significant safety concerns about the long-term risk of cancer following GH administration. Even standard therapeutic GH doses administered to GH deficient children are associated with increased risk of second cancers in some (206-208) but not all (209) follow-up studies although these risks appear largely confined to survivors of childhood cancers and its treatment which render them GH deficient (210-213). Although the significant cancer risk based on uncontrolled observational cohort data using standard GH doses remains contentious (214,215), the long-term risks of much higher GH doses used illicitly by athletes must be viewed with significant concern.
Detection of GH doping remains difficult (216). A major challenge is the non-glycosylated primary structure of recombinant and endogenous 22 kDa GH, that lack the distinctive side-chain carbohydrate differences of exogenous glycoproteins EPO or hCG which provide a convenient basis for sensitive molecular detection tests. Nevertheless, minor infidelities in commercial manufacturing of GH may incorporate distinctive non-natural chemical features proving an exogenous origin (217-219) although these findings have not been developed into detection tests. Challenges to the detection of GH doping arise from the physiological pattern of endogenous GH secretion with its intermittent, pulsatile pattern subject to prominent influence of exercise, stress, and nutritional effects together with GH’s brief circulating half-life and low urine concentrations (220,221). Like other major doping classes, there are both direct and indirect forms of GH doping, involving either direct administration of GH or IGF-I or their analogs and indirect GH doping involving drugs that aim to increase endogenous GH and IGF-I secretion (Table 5).
The first test to detect administration of exogenous GH, the 22kD recombinant form of human GH, was based on blood sampling to measure the ratio of circulating isoforms of GH recognizing the fact that the pituitary secretes not only the major 22 kD isoform (65-80%) but also a variety of minor isoforms including a wide variety of minor isoforms and their multimeric variants (222). Administration of exogenous GH suppresses endogenous pituitary GH secretion leading to a predominance of circulating 22 kD GH. This is the basis for the GH isoform ratio test whereby a serum sample is measured by two different GH immunoassays, one with predominant 22 kD GH specificity (“rec” assay) and the other recognizing the broad spectrum of pituitary GH isoforms (“pit” assay) and the ratio of results (“rec”/”pit” ratio) is an index to detect administration of exogenous recombinant GH (220,223). This ratio test then serves to detect administration of exogenous recombinant human 22kD GH analogous to detection of exogenous T by the urine T/E ratio and exogenous insulin by analysis of serum C peptide (224). The differential GH isoform ratio test has undergone extensive validation involving standardization of the two GH immunoassays with distinctive immunoreactivities to quantify 20kD and 22kD epitopes as well as its application to various populations of elite athletes and evaluating physiological factors which might impact on the validity of test read-out. A strength of this test is that it is aimed at the exogenous doping agent itself, although it cannot definitively distinguish it from its endogenous counterpart. The major limitations of this differential isotope ratio test are its narrow window of detection (24-36 hr post administration) and its inability to detect indirect GH doping. While pituitary-derived human GH might not be detected, human pituitary GH, once obtained from national scale pituitary collection and purification programs, has not been available since 1985 when its risks of Creutzfeldt-Jakob disease were identified (225,226) with recombinant human GH replacing pituitary-extracted GH worldwide. This differential isoform test was first introduced for the 2004 Olympics (227) and led in 2010 to the first successful detection of out of competition GH doping (228).
A complementary detection test with a wider window of detection has been developed based on biomarkers of GH action. This uses two serum biomarkers of tissue GH effects, circulating IGF-1 as a short-term marker of hepatic GH action, and N-terminal peptide of procollagen type III (PIII-NP) as a long-term marker of GH-dependent collagen synthesis. In a study of 102 recreational athletes (53 male, 49 female, mean age 25 years, from 4 different European cities) randomly assigned to self-inject 2.7 mg or 5.4 mg GH or placebo once daily, measurement of serum IGF-1 and PIII-NP by specific immunoassays were able to correctly classify 86% of samples from males and 60% of samples from female using an empirical linear discriminant analysis of log-transformed serum IGF-1 and PIII-NP at the specificity of 1:10,000 required for a WADA biomarker threshold (229). Subsequent studies have shown that additional collagen biomarkers, N-terminal propeptide and C-terminal telopeptide of type I collagen, further widen the window of detection for GH administration (230,231). This multiplex biomarker test, based on using standardized immunoassay antibodies, requires establishment of reliable reference range with specificity (false positive detection rate) of no more than 1:10,000 incorporating the impact of gender and age, although exercise, injury, ethnicity and sports type appear not to be confounding influences but is not yet in routine use by WADA anti-doping labs. The two GH doping test, the differential isoform and biomarker approaches, are considered ultimately complementary (232).